Search Results
We found 14 results for University of Southern California in leadership , webinar , video & news
leadership (1)

Nahyoung Grace Lee, MD
leadership
Harvard Medical School
- Massachusetts Eye and Ear Infirmary
Grace Lee, M.D. is an ophthalmologist at Massachusetts Eye and Ear (MEE) with a rigorous clinical practice in ophthalmic plastic surgery. Approximately 80% of her time is devoted to patient care, which is integrated with teaching residents and fellows in the clinic and surgical setting. This component also includes direct instruction in the wet lab and weekly supervision in the MEE emergency room. Twenty percent of Dr. Lee‘s time is spent doing clinical and basic science research.Dr. Lee completed her BA of Neuroscience at Johns Hopkins University followed by a doctorate in Medicine. Upon completing her ophthalmology residency at the University of Southern California, she pursued a fellowship in ocular oncology and pathology at the Casey Eye Institute, at the Oregon Health & Science University. She directly taught residents in the pathology lab as well as through over 15 hours of didactic lectures. Her additional training involved three years of fellowship in oculoplastic surgery at MEE, where she was the recipient of the Fellow of the Year teaching award. During this fellowship, Dr. Lee collaborated with Dr. Leo Kim to produce an animal model of orbital inflammation and investigated angiogenesis in thyroid eye disease, which was published in Ophthalmology. At the culmination of her training, she was inducted into the American Society of Ophthalmic Plastic and Reconstructive Surgeons (ASOPRS) and is now Assistant Professor of Ophthalmology at Harvard Medical School (HMS).Dr. Lee‘s clinical expertise and innovations have focused on thyroid eye disease and common conditions in ophthalmic plastic surgery. She has expanded her clinical practice to involve anterior segment tumors, building on her fellowship in ocular oncology. In the process, she has trained 4 fellows, 3 of whom have accepted or will be accepting positions at academic institutions. Additionally, she serves as an oral board examiner for the American Board of Ophthalmology.
webinar (8)

Battle of the Medialization Techniques: Michael “Type 1 Thyroplasty” Johns vs. Julina “Reinnervation” Ongkasuwan
webinar
In the next installation of CSurgeries’ series on laryngology, join this interactive webinar with Dr. Julina Ongkasuwan, associate professor of adult and pediatric laryngology at Baylor College of Medicine, and Dr. Michael Johns, Director, USC Voice Center and Professor, Caruso Department of Otolaryngology – Head and Neck Surgery – University of Southern California, for a discussion of permanent medialization techniques. Type 1 thyroplasty vs Reinnervation.
Which one will you choose and when?
Pediatric Endoscopic Airway Surgery
webinar
This webinar will address common and advanced pediatric airway pathology. There will be a focus on video demonstration of advanced surgical endoscopic management of pediatric airway pathology ranging from laryngomalacia to type 3 laryngeal clefts.

Vikash K. Modi, MD, is an Associate Professor and the Chief of Pediatric Otolaryngology - Head & Neck Surgery at New York Presbyterian Hospital- Weill Cornell Medical Center. After receiving his medical degree from the Rutgers Medical School, Dr. Modi completed his residency in Otolaryngology at the University of Southern California - Keck School of Medicine. Following residency, Dr. Modi completed a Pediatric Otolaryngology fellowship at Northwestern University - Children's Memorial Hospital. He founded the Cornell Aerodigestive Center and has one of the largest series of endoscopic posterior cricoid split with rib grafting (presented at ESPO). He also has presented his work on endoscopic repair of laryngeal clefts at ASPO and CEORL. He has been inducted as a Fellow, into the prestigious Triological Society for his thesis paper on airway balloon dilation and currently serves as a Section Editor-Video Editor of The Laryngoscope and is known for his surgical endoscopic airway videos.

A Discussion About Removal of Intraocular Foreign Bodies
webinar
Attendees will learn about the proper procedure to follow when removing foreign bodies from the eye by discussing the process with three expert Vitreoretinal Surgeons.
Mitul Mehta, MD, MS
Fellowship Director of Vitreoretinal Surgery / Health Sciences Clinical Associate Professor
Gavin Herbert Eye Institute / University of California, Irvine
Mitul Mehta MD MS, is a board-certified ophthalmologist with fellowship training in medical and surgical diseases of the retina. He sees patients at the UCI Medical Center in Orange, CA and the Gavin Herbert Eye Institute in Irvine, CA. Dr. Mehta graduated from the Massachusetts Institute of Technology (MIT), he then completed a Master of Science degree in Physiology & Biophysics at Georgetown University and earned his MD degree from the University of Southern California (USC). After completing his ophthalmology residency at the University of Cincinnati, he graduated from fellowship training in vitreoretinal surgery at the New York Eye & Ear Infirmary of Mount Sinai. Dr. Mehta cares for patients with vitreoretinal disorders as the Vitreoretinal Surgery Fellowship Director. He teaches medical students, residents, and fellows, and does research in surgical devices, techniques and vitreoretinal diseases such as retinitis pigmentosa, diabetic retinopathy and macular degeneration.

C. Kiersten Pollard, MD
Vitreoretinal Surgeon
The Retina Center of Western Colorado
Dr. Pollard completed her undergraduate education at the Massachusetts Institute of Technology, she then went on to earn her MD at the University of Colorado School of Medicine where she also completed her intern year in internal medicine. She completed her Ophthalmology residency at the University of Arizona and her vitreoretinal surgery fellowship at UT Southwestern Medical Center. Dr. Pollard practices at The Retina Center of Western Colorado where she and her partners provide advanced medical and surgical vitreoretinal care to the people of western Colorado, eastern Utah, and southern Wyoming.

Hemang K. Pandya, MD FACS
Vitreoretinal Specialist / President
Dallas Retina Center / American Retina Forum
Dr. Pandya earned his M.D., with Alpha Omega Alpha honors, from the Chicago Medical School. Dr. Pandya completed his Ophthalmology training at the Kresge Eye Institute. Thereafter, Dr. Pandya completed a 2-year fellowship in Vitreoretinal Surgery at the Dean McGee Eye Institute. Dr Pandya practices at Dallas Retina Center and can be reached at DrPandya@DallasRetina.com.
Pre-Operative Planning, Intraoperative Considerations and Troubleshooting
webinar
In this first Cardiothoracic DocTalk session of the Pathway to Independence for Junior Surgeons we will discuss Redo Sternotomy and Pulmonary Valve Replacement in a patient who had prior TOF repair. We plan to highlight the pre-operative strategy which will include necessary imaging and testing along with how to manage an intra-operative complication of air embolism. Viewers of this webinar will gain valuable insight into a stepwise approach to managing a very complex surgical scenario.

Lawrence Greiten, MD
Assistant Professor in Division of Congenital Cardiac Surgery
Arkansas Children's Hospital (ACH) and the University of Arkansas for Medical Sciences (UAMS)
Lawrence Greiten, M.D., is an Assistant Professor in the Division of Congenital Cardiac Surgery at Arkansas Children’s Hospital (ACH) and the University of Arkansas for Medical Sciences (UAMS). Dr. Greiten received his undergraduate degree from Kansas Wesleyan University and his medical degree from the University Of Arizona College Of Medicine. He completed both his General Surgery training and Cardiovascular and General Thoracic Surgery fellowship at the Mayo School of Graduate Medical Education, where he also earned a Masters in Biomedical Sciences, Clinical and Translational Science. He did an advanced Fellowship in Congenital Cardiac Surgery at Children’s Hospital Los Angeles, Keck Medical School at the University of Southern California.
Surgical Exposure, Minimal Incision Surgical Option for ASD Repair
webinar
In this second Cardiothoracic DocTalk session of the Pathway to Independence for Junior Surgeons we plan to discuss the approach to a Minimal Incision ASD. Our panel will discuss the merits of offering this approach along with the potential pitfalls. Viewers of this webinar will gain insight into optimizing surgical exposure and understanding when it is safe to proceed with less invasive techniques.
Lawrence Greiten, MD
Assistant Professor in Division of Congenital Cardiac Surgery
Arkansas Children's Hospital (ACH) and the University of Arkansas for Medical Sciences (UAMS)
Lawrence Greiten, M.D., is an Assistant Professor in the Division of Congenital Cardiac Surgery at Arkansas Children’s Hospital (ACH) and the University of Arkansas for Medical Sciences (UAMS). Dr. Greiten received his undergraduate degree from Kansas Wesleyan University and his medical degree from the University Of Arizona College Of Medicine. He completed both his General Surgery training and Cardiovascular and General Thoracic Surgery fellowship at the Mayo School of Graduate Medical Education, where he also earned a Masters in Biomedical Sciences, Clinical and Translational Science. He did an advanced Fellowship in Congenital Cardiac Surgery at Children’s Hospital Los Angeles, Keck Medical School at the University of Southern California.
Surgical Pitfalls, Early Career Advancement and Leadership
webinar
In this last Cardiothoracic DocTalk session of the Pathway to Independence for Junior Surgeons we will discuss early career mistakes and how to avoid them. Viewers of this webinar will learn tips and tricks learned from senior partners and knowing when to call for help.
Lawrence Greiten, MD
Assistant Professor in Division of Congenital Cardiac Surgery
Arkansas Children's Hospital (ACH) and the University of Arkansas for Medical Sciences (UAMS)
Lawrence Greiten, M.D., is an Assistant Professor in the Division of Congenital Cardiac Surgery at Arkansas Children’s Hospital (ACH) and the University of Arkansas for Medical Sciences (UAMS). Dr. Greiten received his undergraduate degree from Kansas Wesleyan University and his medical degree from the University Of Arizona College Of Medicine. He completed both his General Surgery training and Cardiovascular and General Thoracic Surgery fellowship at the Mayo School of Graduate Medical Education, where he also earned a Masters in Biomedical Sciences, Clinical and Translational Science. He did an advanced Fellowship in Congenital Cardiac Surgery at Children’s Hospital Los Angeles, Keck Medical School at the University of Southern California.
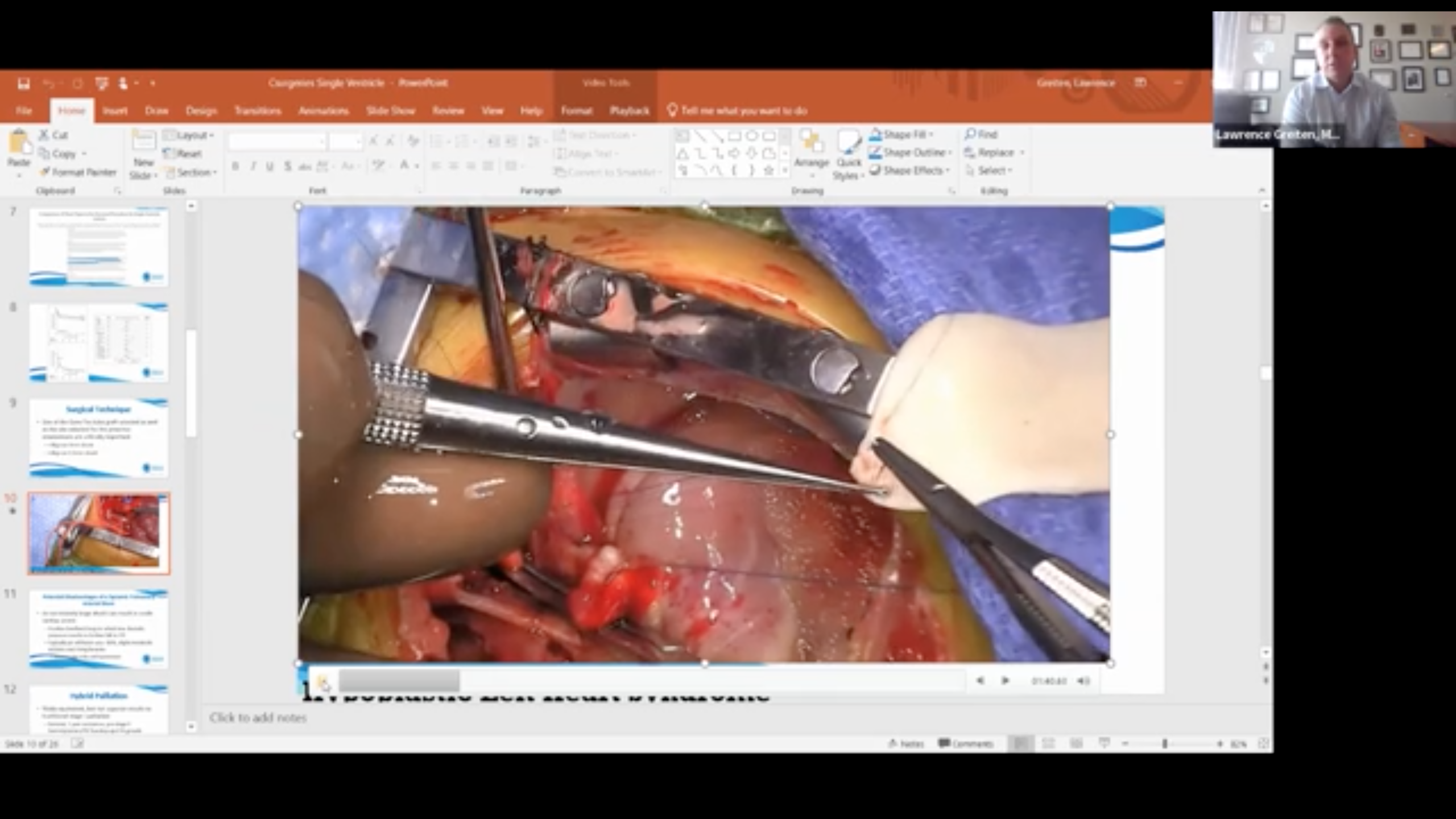
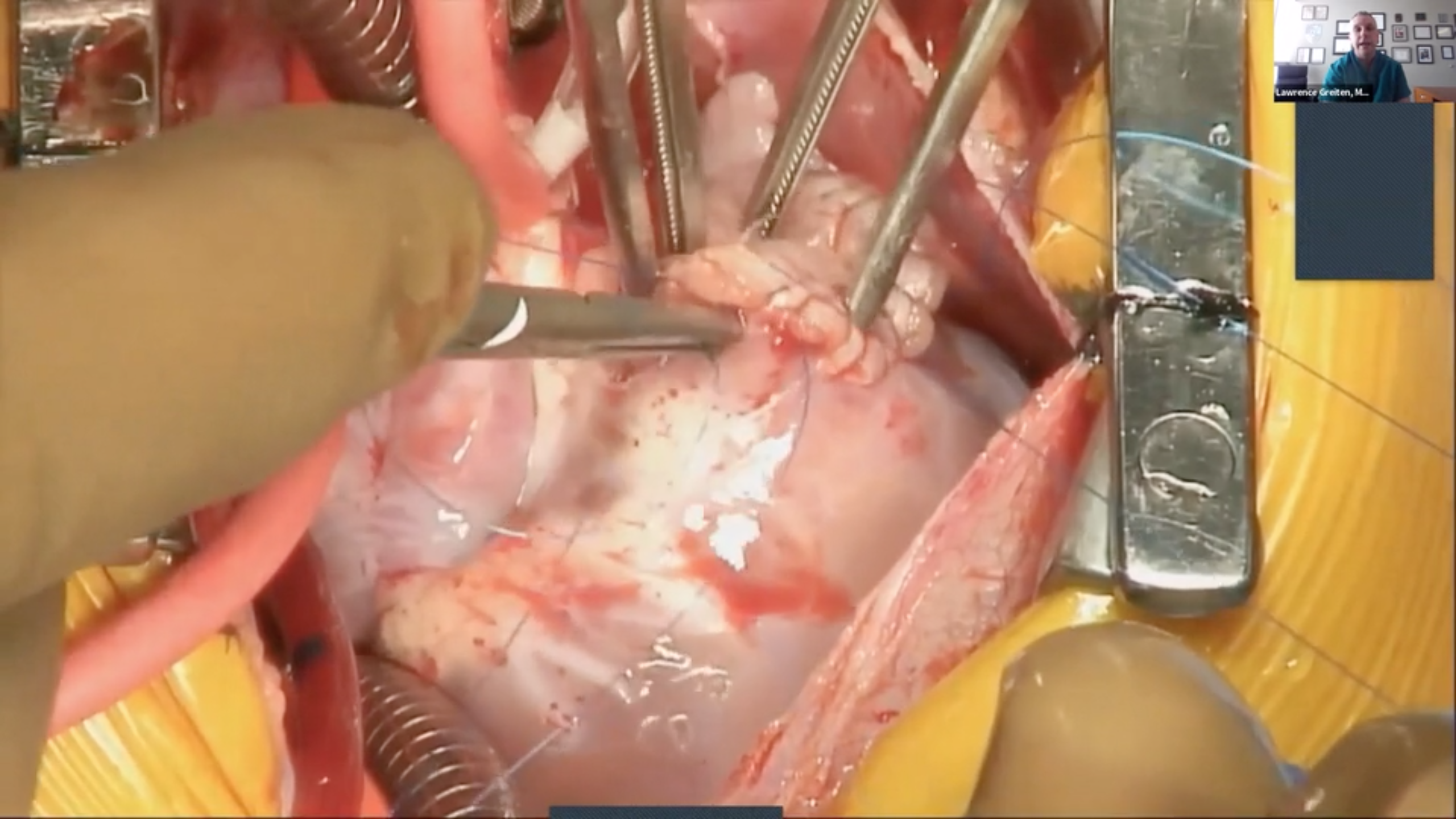
Three Stage Management of the Single Ventricle
webinar
In this session our team of experts will discuss the three stages of single ventricle palliation including the Norwood procedure, the bidirectional Glenn shunt and the Fontan procedure. Included in this webinar will be single ventricle pathophysiology, diagnostic studies/imaging, indications and contraindications for palliation, timing of surgical intervention, and overview of surgical goals and associated mortality.


Assistant Professor in Division of Congenital Cardiac Surgery
Arkansas Children's Hospital (ACH) and the University of Arkansas for Medical Sciences (UAMS)
Lawrence Greiten, M.D., is an Assistant Professor in the Division of Congenital Cardiac Surgery at Arkansas Children’s Hospital (ACH) and the University of Arkansas for Medical Sciences (UAMS). Dr. Greiten received his undergraduate degree from Kansas Wesleyan University and his medical degree from the University Of Arizona College Of Medicine. He completed both his General Surgery training and Cardiovascular and General Thoracic Surgery fellowship at the Mayo School of Graduate Medical Education, where he also earned a Masters in Biomedical Sciences, Clinical and Translational Science. He did an advanced Fellowship in Congenital Cardiac Surgery at Children’s Hospital Los Angeles, Keck Medical School at the University of Southern California.
Research Intern
Arkansas Children’s Research Institution / University of Arkansas for Medical Sciences
Sophia is a Pre-Medical Track student that recently graduated with a traditional BA-Biology degree and a minor in Medical Humanities. She is always seeking to expand her knowledge and gain exposure to pediatric research in hopes of bettering herself as an aspiring physician and continuing research in the future.


CVOR Surgical Assistant Chief
Arkansas Children's Hospital
Over 28 years of adult and congenital heart surgery experience. I have helped develop a minimally invasive and robotic surgery program at UCLA. In addition, I have been involved with Ex-Vivo heart and lung preservation trials and several drug trials.
Professor, Department of Surgery / Director, Heart Institute
UAMS College of Medicine / Arkansas Children’s Hospital
Brian Reemtsen, M.D. is a Professor at the University of Arkansas for Medical Sciences in the Division of Pediatric Cardiothoracic Surgery at Arkansas Children’s Hospital. He is also Director of the Heart Institute at Arkansas Children’s Hospital. He received his undergraduate degree from the University of California at Los Angeles (UCLA), and his medical degree from New York Medical College. He completed his internship and residency at UCLA School of Medicine. He then completed fellowships at the University of Washington, as well as the Great Ormond Street Hospital in London, England.

Pediatric Cardiologist
Arkansas Children's Hospital
After completion of her formal training, Dala Zakaria, M.D., joined the faculty of the University of Arkansas for Medical Sciences in 2013, practicing at Arkansas Children’s. Her primary clinical interests are transesophageal and fetal echocardiography, and advanced imaging, including 3D. Dr. Zakaria performs and interprets transthoracic and transesophageal echocardiograms in our outpatient, inpatient and telemedicine programs. She is an integral part of the Fetal Echocardiography program, providing fetal echocardiogram interpretation and consultation.

Ventricular Septal Defects
webinar
As one of the most common congenital cardiac anomalies managed by pediatric cardiac teams, VSD’s often may present a challenge in optimal management. Our team of experts will discuss pathophysiology, diagnostic studies, indications and timing of surgery, surgical management; along with the technical challenges/considerations of repairing each of the different anatomic variants of ventricular septal defects: perimembranous, conoventricular, supracristal (subpulmonary), inlet (atrioventricular canal type), and muscular.
Assistant Professor in Division of Congenital Cardiac Surgery
Arkansas Children's Hospital (ACH) and the University of Arkansas for Medical Sciences (UAMS)
Lawrence Greiten, M.D., is an Assistant Professor in the Division of Congenital Cardiac Surgery at Arkansas Children’s Hospital (ACH) and the University of Arkansas for Medical Sciences (UAMS). Dr. Greiten received his undergraduate degree from Kansas Wesleyan University and his medical degree from the University Of Arizona College Of Medicine. He completed both his General Surgery training and Cardiovascular and General Thoracic Surgery fellowship at the Mayo School of Graduate Medical Education, where he also earned a Masters in Biomedical Sciences, Clinical and Translational Science. He did an advanced Fellowship in Congenital Cardiac Surgery at Children’s Hospital Los Angeles, Keck Medical School at the University of Southern California.
Research Intern
Arkansas Children’s Research Institution / University of Arkansas for Medical Sciences
Sophia is a Pre-Medical Track student that recently graduated with a traditional BA-Biology degree and a minor in Medical Humanities. She is always seeking to expand her knowledge and gain exposure to pediatric research in hopes of bettering herself as an aspiring physician and continuing research in the future.
CVOR Surgical Assistant Chief
Arkansas Children's Hospital
Over 28 years of adult and congenital heart surgery experience. I have helped develop a minimally invasive and robotic surgery program at UCLA. In addition, I have been involved with Ex-Vivo heart and lung preservation trials and several drug trials.
Professor, Department of Surgery / Director, Heart Institute
UAMS College of Medicine / Arkansas Children’s Hospital
Brian Reemtsen, M.D. is a Professor at the University of Arkansas for Medical Sciences in the Division of Pediatric Cardiothoracic Surgery at Arkansas Children’s Hospital. He is also Director of the Heart Institute at Arkansas Children’s Hospital. He received his undergraduate degree from the University of California at Los Angeles (UCLA), and his medical degree from New York Medical College. He completed his internship and residency at UCLA School of Medicine. He then completed fellowships at the University of Washington, as well as the Great Ormond Street Hospital in London, England.


Assistant Professor, Pediatric Cardiology & Radiology
University of Arkansas for Medical Sciences / Arkansas Children’s Hospital
Dr. Merves is a pediatric cardiologist with a specific interest and additional training in cardiac imaging. In clinical practice, she cares for patients across all age ranges from fetal life through adulthood and performs and interprets fetal echocardiograms, transthoracic and transesophageal echocardiograms, cardiac MRIs and cardiac CTs. She has an interest in imaging related research and education.
Pediatric Cardiologist / Associate Professor of Pediatrics / Pediatric Cardiology Fellowship Program Director
University of Arkansas for Medical Sciences / Arkansas Children’s Hospital
Dr. Daily is a non-invasive pediatric cardiologist who serves as the Pediatric Cardiology Fellowship Program Director at Arkansas Children’s Hospital. His interests include echocardiography, adult education, and physician personal finance.
video (4)

Retroseptal Transconjunctival Approach to Orbital Floor Blowout Fracture
videoThe transconjunctival approach was first described by Bourquet in 1924 and then modified by Tessier in 1973 for exposure of the orbital floor and maxilla for the treatment of facial trauma. This approach can be carried out either in a preseptal plane by separating the orbital septum from within the eyelid (preseptal approach) or posterior to the septum and eyelid (retroseptal approach) by making an incision through the bulbar conjunctiva directly above the orbital rim. The main advantage of the retroseptal approach is that it does not involve dissection and disruption of the eyelid itself, therefore, reducing the incidence of post-operative lid laxity and position abnormalities. This video will show a retroseptal approach to an orbital floor blowout fracture. A lateral inferior cantholysis is performed to facilitate eversion and retraction of the lower eyelid.
EMG Guided Botulinum Toxin Injection for Adductor Spasmodic Dysphonia
videoContributors: Christian Lava, Hagit Shoffel-havakuk, and Michael M Johns Iii Adductor spasmodic dysphonia is the most common form of laryngeal dystonia, causing inappropriate glottic closure and strangled choppy voice. This video demonstrates step by step, the standard treatment for adductor spasmodic dysphonia: bilateral, EMG-guided, percutaneous botulinum toxin injections to the TA-LCA (thyroarytenoid and lateral cricoarytenoid) muscles.
Treatment of Adult Idiopathic Subglottic Stenosis with CO2 Laser and Balloon Dilation
videoContributors: Michael M. Johns III and Benjamin Anthony The patient is a 53 year-old female with history of idiopathic subglottic stenosis and long-standing right vocal fold scarring who had previously been treated endoscopically in the operating room and in the office with steroid injections. She returns to the operating room for scheduled endoscopic CO2 laser treatment, Depo-Medrol injection (not shown), balloon dilation, and Mitomycin C application (not shown). DOI: http://dx.doi.org/10.17797/p7s4gn9n20 Editor Recruited By: Michael M. Johns, III, MD
Awake Steroid Injection for Idiopathic Subglottic Stenosis
videoContributor: Michael Johns III, MD This video demonstrates a steroid injection in an awake patient for the treatment of idiopathic subglottic stenosis. The patient is first anesthetized with topical 2% lidocaine over the larynx and 1% lidocaine with epinephrine percutaneously over the cricoid cartilage. An endoscope is passed transnasally and positioned just below the vocal folds. A 23 gauge needle is then passed through the cricothyroid membrane, and Kenalog is circumferentially injected submucosally taking care not to reduce the caliber size of the airway. DOI: http://dx.doi.org/10.17797/htvmbepobg
news (1)

Meet our Presenters for Day 2!
news
The International Adult Airway Symposium is coming up this weekend! For more information view the itinerary or register here!
Dr. Vyvy Young
Associate Professor and the Associate Residency Program Director in the Department of Otolaryngology-Head and Neck Surgery
University of California – San Francisco
VyVy Young, MD, is an Associate Professor and the Associate Residency Program Director in the Department of Otolaryngology-Head and Neck Surgery at the University of California – San Francisco. Dr. Young received her undergraduate and medical degrees from the University of Louisville, in Louisville, Kentucky, where she also pursued her Otolaryngology training. She then completed a fellowship in Laryngology and Care of the Professional Voice at the University of Pittsburgh Voice Center. She currently serves the American Academy of Otolaryngology – Head and Neck Surgery as member of the Annual Meeting Program Committee and Executive Committee for ENThealth.org. She is immediate past-chair of the Voice Committee and the Women in Otolaryngology Communications Committee and was recently selected as chair of the Finance and Audit Committee of the American Broncho-Esophagological Association.

Justin Roe, PhD, FRCSLT
Clinical Service Lead - Speech and Language Therapy – National Centre for Airway Reconstruction
Imperial College Healthcare NHS Trust
Dr. Roe is a clinical-academic and service lead, specialising in dysphagia in benign and malignant head and neck disease. He leads the speech and language therapy service for the National Centre for Airway Reconstruction at Imperial College Healthcare NHS Trust and is a consultant and service lead at the Royal Marsden NHS Foundation Trust. He is an Honorary Clinical Senior Lecturer at Imperial College London and an investigator on a number of NIHR portfolio studies. He is currently on an NIHR Imperial Biomedical Research Centre/ Imperial Health Charity funded post-doctoral research fellowship. He is an elected council member for the British Laryngological Association and British Association of Head and Neck Oncologists.

Professor Anil Patel MBBS PhD FRCA
Clinical Anaesthetist / Chairman of Department of Anaesthesia
Royal National ENT & Eastman Dental Hospital
Professor Anil Patel graduated from University College London in 1991. He is a clinical anaesthetist and continues to develop and refine the largest experience of anaesthetising adult airway patients under general anaesthesia (> 6,000 procedures) in the UK, probably Europe and possibly the world. His research interests include all aspects of shared airway and difficult airway management. Professor Patel has been an invited speaker to over 300 national and international meetings in 38 countries. He has over 130+ peer reviewed publications, 25 book chapters, over 4,500 citations and an h-index of 25.

Robbi A. Kupfer, MD
Associate Professor, Department of Otolaryngology-Head & Neck Surgery
University of Michigan
Dr. Kupfer is an Associate Professor of Otolaryngology-Head & Neck Surgery at the University of Michigan who specializes in Laryngology and Bronchoesophagology. She is the Program Director for the Laryngology Fellowship as well as the Otolaryngology Residency at the University of Michigan.

Alexander T. Hillel, MD, FACS
Associate Professor
Johns Hopkins University School of Medicine
Dr. Alexander Hillel is a Laryngologist, Residency Program Director, and Vice Director of Education in the Johns Hopkins Department of Otolaryngology – Head & Neck Surgery. His clinical practice and research centers on the treatment, prevention, and causes of laryngotracheal stenosis (LTS).

Dale Ekbom, MD
Associate Professor of Otolaryngology / Director of Voice Disorders/Laryngology
Mayo Clinic
Residency in Otolaryngology/Head and Neck Surgery at the University of Michigan with a fellowship in Laryngology/Care of the Professional Voice at Vanderbilt University Medical Center. Clinically specializing in voice, especially management of vocal fold paralysis, Zenker’s diverticulum and Cricopharyngeal muscle dysfunction, early laryngeal cancer, and airway compromise due to laryngeal, subglottic, and tracheal stenosis. Research interests include idiopathic subglottic stenosis and GPA with surgical and medical management of the airway, vocal fold paralysis, new injectables using Jellyfish collagen.

Dr. Ricky Thakrar
Consultant Chest Physician
University College London Hospital
Dr. Ricky Thakrar qualified in Medicine from Imperial College London. He trained in Respiratory Medicine at the Royal Brompton Hospital and completed his training in Northwest London. He was appointed to a three-year academic fellowship at UCL where his PhD examined state of the art bronchoscopy techniques for managing cancers arising in central airways and lung. He is a Consultant in Thoracic Medicine and his main interests are in interventional bronchoscopy procedures (laser resection, airway stenting, cryotherapy, photodynamic therapy and brachytherapy) for pre-malignant and malignant disease of the tracheobronchial tree.

Dr. Michael Rutter
Director of the Aerodigestive Center
Cincinnati Children's Hospital
Dr. Rutter is an ENT surgeon specializing in pediatric otolaryngology with an emphasis on airway problems in children, adolescents and young adults. His interests include tracheal reconstruction and complex airway surgery. Always a problem-solver, he strives to involve the patient in their own care by having them help evaluate the issue and then craft a solution together. He was drawn to his career by the challenge and highly individualized nature of pediatric airway problems and management. Dr. Rutter enjoys working in a multidisciplinary team setting and focusing on coordinated care for complex childhood airway conditions. He was honored to receive the 2016 Gabriel Frederick Tucker Award from the American Laryngological Association, and the 2018 Sylvan Stool Teaching Award from the Society for Ear Nose and Throat Advancement in Children (SENTAC). These awards are for his contributions to the field of pediatric laryngology. In addition to caring for patients, he is also dedicated to his research trying to find improvements in airway management.

Christopher T. Wootten, MD, MMHC
Director, Pediatric Otolaryngology—Head and Neck Surgery
Vanderbilt University Medical Center
Dr. Wootten has a longstanding interest in surgical management of congenital and acquired airway disorders. To better equip himself to lead the Pediatric ENT service through expansion, evolution of practice models, and differentiation into multidisciplinary care, Dr. Wootten obtained a Masters of Management in Health Care at Vanderbilt’s Owen School of Business in 2017. Areas of his professional research emphasis include airway obstruction in children and adults and aerodigestive care. He innovates minimally invasive surgical techniques in the head and neck. Dr. Wootten is actively investigating the role of eosinophil and mast cell-based inflammation in the pediatric larynx.

Karla O'Dell, M.D.
Assistant Professor / Co-director
USC Voice Center, Caruso Department of Otolaryngology Head and Neck Surgery @ University of Southern California / USC Center for Airway Intervention and Reconstruction
Karla O’Dell, MD, specializes in head and neck surgery and disorders of the voice, airway and swallowing. She is cofounder and codirector of the USC Airway Intervention & Reconstruction Center (USC Air Center).

Jeanne L. Hatcher, MD, FACS
Co-Director of the Emory Voice Center and Associate Professor of Otolaryngology
Emory University School of Medicine
Dr. Hatcher has been at Emory since 2014 after completing her laryngology fellowship with Dr. Blake Simpson; she specializes in open and endoscopic airway surgery as well as voice disorders. Dr. Hatcher is a member of the ABEA and post-graduate member of the ALA and also serves on the Ethics and Voice Committees for the American Academy of Otolaryngology Head and Neck Surgery.

Mr. Lee Aspland
Patient / Freelance Artist
Lee Aspland Photography
Lee Aspland is a photographer, author and mindful practitioner who creates photography that reflects his feelings about living in such a glorious world. He specializes in Mindful Photography, capturing a fleeting feeling or thought, a hope or fear, a frozen single moment in time.

Gemma Clunie, MSc, BA (Hon), MRCSLT
Clinical Specialist Speech-Language Pathologist (Airways/ENT) and HEE/NIHR Clinical Doctoral Research Fellow
Imperial College Healthcare NHS Trust/ Imperial College London, Department of Surgery & Cancer
Gemma is a Clinical Specialist Speech and Language Therapist with an interest in voice and swallowing disorders that is particularly focused on the benign ENT, head and neck, respiratory and critical care populations. Gemma is a current NIHR/HEE Clinical Doctoral Research Fellow at Imperial College London. Her PhD studies focus on the voice and swallowing difficulties of airway stenosis patients. She is based at Charing Cross Hospital in London where she has worked for the last six years as part of the National Centre for Airway Reconstruction, Europe’s largest centre for the management of airway disorders.

Niall C. Anderson, CPsychol, MSc, BSc
Lead Psychologist (formerly Respiratory Highly Specialist Health Psychologist)
Bart's Health NHS Trust (formerly Central & North West London NHS Foundation Trust)
Niall is a HCPC Registered & BPS Chartered Practitioner Health Psychologist, and BPS RAPPS Registered Supervisor. Niall has specialist experience of working within healthcare systems with people with long-term health conditions at all system levels to support physical, psychological and social wellbeing. Niall worked in the Airway Service at Charing Cross Hospital (London, UK) between January-December 2021 in order to develop and implement the Airway Psychology Service.
